
Hi folks! Caroline here from SchrothDC. I’m stepping up on my soapbox today to discuss a commonly prescribed movement that is driving me nuts in the clinic.
The posterior pelvic tilt, or “tucking of the tailbone”, has somehow become a panacea for all low back issues. People get this advice ALL THE TIME – in physical therapy, yoga, pilates, barre, and many other places. Full disclosure: I handed out this advice all the time before I did my Schroth training. Why? General physical therapists and fitness instructors equate this advice to:
A) Increasing core strength and
B) Decompressing the low back/separating the facet joints
Ok, so why has the posterior pelvic tilt become the villain in my life as of late?
Don’t get me wrong, there are hyperlordotic bodies out there who do need this advice. (Hyperlordotic means you have a giant arch in your low back).

But what about those of us who have flat backs, or a loss of the natural lumbar curvature (i.e. lordosis)? (me, me, me, me, me! I don’t have scoliosis but I am hypermobile, which also causes flatback). If our tailbones are already in a tucked-under position, why would we tuck under more, further exacerbating our flatbacks?

If we acknowledge that our bodies are all built a little differently, we know that we will all need slightly different exercise instruction.
This is why I’m so amped up about this: Lumbar scoliosis is a thief of lumbar lordosis.
Many of our patients with lumbar scoliosis come to us after having seen one or more general physical therapists, who have prescribed a slew of tailbone tucking exercises – single knee to chest, double knee to chest, child’s pose, pelvic tilts against the wall, forward folds, sit-ups, etc. What we’ve found is that we have to undo the advice they’ve previously received, which can be shocking to the patient. Some of these patients have been tucking their tailbones for decades! Even more mind-blowing to them is that we teach them how to lift their tailbones (i.e. anterior pelvic tilt), the exact opposite of what they’ve been practicing.
Anyone who walks into our clinic with lumbar scoliosis will never; I repeat NEVER, be asked by us to do a posterior pelvic tilt. The goal of the Schroth Method is to restore the natural lumbar lordosis and preserve that natural curvature over the lifespan. Tucking the tailbone under will undermine our efforts to elongate and erect the rest of the spine.
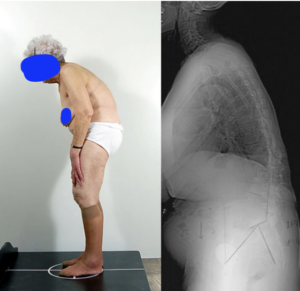
This concept is especially important in adulthood. Many studies have investigated the adult scoliosis population’s predictors of pain and disability. Across multiple studies, the loss of lumbar lordosis/flattened low back is the main contributor to pain and disability.¹ Furthermore, the loss of lumbar lordosis sets off a chain of compensatory mechanisms in the body – kyphotozation of the thoracolumbar junction, leading to thoracic hyperkyphosis, leading to pelvis retroversion, leading to knee flexion – which results in trunk collapse.²
Here’s your try this at home for the month: sit in a chair (if you’re not already). Tuck your tailbone under, then try to get as tall as you can. Now roll the pelvis in the opposite direction so your SITS bones are rooted firmly into the chair and your low back has a little arch, and then get as tall as you can. Can you feel the difference? The latter exercise (non-tucked) should be a very obvious winner in terms of upright, tall posture.
So to all my flat-back friends, whether it be a product of scoliosis or run-of-the-mill hypermobility, please, please, please, start lordot-ing. Your spine will thank you for it.
-
Schwab, F; Adult Scoliosis a Quantitative Radiographic and Clinical Review. Spine, 2002. Vol. 27, No. 4:387-392.
Hong et al. The Prevalence and radiological findings in 1347 elderly patients with scoliosis. J Bone Joint Surg. Br. July;9(7):980-3
-
Barrey C, Roussoully P, Le Huec JC, D’Acunzi G, Perrin G. Compensatory mechanisms contributing to keep sagittal balance of the spine. Eur Spine J. 2013;22(Suppl 6):834-841.